Cardiopulmonary resuscitation (CPR) is an emergency procedure designed to maintain some blood flow to the heart and brain in a person who is in cardiac arrest. It involves the combination of chest compressions and artificial ventilation to provide oxygen to the body’s vital organs when normal breathing and heart function have stopped.
The origins of CPR trace back to the early 18th century when various techniques were attempted, including blowing smoke into the rectum, or using bellows to stimulate breathing. However, the modern concept of CPR was developed in the mid-20th century.
Kouwenhoven Method: Dr. James Elam and Dr. Peter Safar pioneered the “mouth-to-mouth” resuscitation technique in the 1950s.
Cardiac Massage: Dr. Peter Safar and Dr. James Jude further developed CPR, combining chest compressions with artificial ventilation, known as the “cardiac massage” technique.
CPR as We Know It: In 1960, the American Heart Association (AHA) endorsed the “mouth-to-mouth” method, which soon evolved into the combination of chest compressions and rescue breathing that we recognize as CPR today.
AHA Guidelines: The AHA continues to update guidelines for CPR based on scientific research. They emphasize high-quality chest compressions and early defibrillation in cases of sudden cardiac arrest.
CPR is taught and practiced worldwide, saving countless lives each year. Its fundamental goal is to buy time for professional medical assistance to arrive and provide advanced care for those experiencing cardiac arrest.
Indications
Cardiac Arrest: CPR is performed in cases of sudden cardiac arrest, where the heart’s electrical activity becomes chaotic or stops altogether. This can be due to various factors, such as a heart attack, arrhythmias, or other cardiac issues.
Respiratory Arrest: If a person experiences a complete cessation of breathing (respiratory arrest), it is essential to initiate CPR to ensure oxygen is delivered to vital organs, including the brain.
Drowning: In cases of near-drowning or drowning victims, CPR should be initiated immediately if the person is unresponsive and not breathing.
Choking: If a person’s airway is obstructed by a foreign object and results in unconsciousness, CPR is required once the airway is cleared.
Drug Overdose: In the event of a severe drug overdose or poisoning that leads to unconsciousness and loss of breathing or a pulse, CPR may be necessary.
Electrocution: Victims of electrical shock can experience cardiac arrest. CPR should be performed if the person is unresponsive and not breathing.
Suffocation: Cases of suffocation or strangulation may cause unconsciousness and respiratory or cardiac arrest. CPR is required in these situations.
Severe Allergic Reaction (Anaphylaxis): In rare cases, severe allergic reactions (anaphylaxis) can lead to cardiac arrest. CPR should be performed if the person becomes unresponsive and loses a pulse.
Trauma: In traumatic injuries that result in cardiac or respiratory arrest, such as severe head injuries, chest injuries, or accidents causing significant blood loss, CPR may be indicated.
Contraindications
Obvious Signs of Death: If a person has been dead for an extended period, such as rigor mortis (stiffening of the body) or obvious signs of decomposition, resuscitative efforts are unlikely to be effective. In such cases, it may not be appropriate to initiate CPR.
Do-Not-Resuscitate (DNR) Orders: If the person has a valid and properly documented DNR order, healthcare providers and bystanders are legally obligated to respect the patient’s wishes. DNR orders specify that the person does not wish to receive CPR or other resuscitative measures in the cardiac events or respiratory arrest.
Decomposed Body: In cases where the body is significantly decomposed, CPR is unlikely to be effective, and it may not be indicated.
Futility: If there is clear evidence that resuscitation is futile and unlikely to result in a successful outcome, such as severe head trauma with a fixed and dilated pupil, continuing CPR may not be appropriate.
Injuries Incompatible with Life: In some traumatic injuries, such as a complete decapitation, where there is no potential for survival, CPR may be contraindicated.
Outcomes
Return of Spontaneous Circulation (ROSC): The primary goal of CPR is to reestablish a heartbeat and circulation. When CPR is administered promptly and effectively, some individuals may achieve ROSC. This means that their heart starts beating again, and they have a return of vital signs.
Survival to Hospital Admission: Some patients who receive CPR may survive long enough to be admitted to a hospital. The chances of survival increase when high-quality CPR is combined with rapid defibrillation and advanced cardiac life support.
Survival to Hospital Discharge: The goal of CPR is for the patient to survive and be discharged from the hospital with a good neurological outcome. However, this outcome is achieved in a smaller percentage of cases and often depends on factors such as the initial cause of cardiac arrest and the duration of CPR.
Neurological Outcomes: For those who survive cardiac arrest, the quality and duration of CPR, as well as the rapidity of advanced care, can influence their neurological outcome. Some survivors may experience minimal or no neurological deficits, while others may have varying degrees of cognitive or physical impairment.
No ROSC or Survival: Unfortunately, not all patients who receive CPR will achieve ROSC or survive. In some cases, the underlying cause of cardiac arrest is too severe, or CPR is not administered in time to be effective. The decision to terminate CPR may be made in cases where resuscitative efforts are deemed futile.
Complications: CPR can be physically demanding and may lead to complications such as rib fractures, lung injuries, and damage to internal organs. While these complications are possible, they are considered acceptable risks given the life-threatening nature of cardiac arrest.
Equipment
Protective Gear: Before initiating CPR, ensure you are wearing protective equipment such as gloves and a face shield to reduce the infection transmission and ensure your safety.
Automated External Defibrillator (AED): If available, use an AED to analyze the patient’s heart rhythm and deliver electric shocks if needed. These devices are user-friendly and provide voice prompts for guidance.
CPR Barrier Device: This is a one-way valve mask used to provide rescue breaths while preventing direct contact between the rescuer and the patient’s mouth.
Patient Positioning
Safety: Ensure the safety of the rescuer and bystanders by assessing the scene for potential dangers. If the environment is unsafe, wait for professionals to arrive or ensure the area is secure before beginning CPR.
Position on a Firm Surface: Lay the patient on a firm, flat surface to provide effective chest compressions. For adults and children, this is typically the ground or a hard floor. For infants, a table or countertop may be suitable.
Supine Position: The patient should be in a supine position (lying on their back) for CPR. This position allows for easier access to the chest for chest compressions and the application of an AED.
Clear the Chest: Ensure the patient’s chest is clear of any obstacles, clothing, or items that may interfere with chest compressions.
Adequate Exposure: For effective chest compressions, the patient’s chest should be exposed. Remove any clothing that covers the chest if necessary.
Correct Hand Placement: For adult CPR, position the heel of one hand on the center of the chest, just below the nipple line. Place the other hand on top of the first hand, interlocking the fingers. For children and infants, use one hand or two fingers, respectively.
AED Attachment: If an AED is available, attach the electrode pads to the patient’s chest as per the manufacturer’s instructions. These pads typically have visual aids for proper placement.
TECHNIQUE
Step-1: Assess the Scene
Ensure the safety of yourself, the victim, and any bystanders.
If the scene is safe, approach the victim and check for responsiveness by tapping and shouting, “Are you okay?”
Step-2: Call for Help
If the victim is unresponsive, immediately call emergency services or ask a bystander to do so.
Step-3: Check for Normal Breathing
Place your ear near the victim’s mouth and nose to listen and feel normal breathing (not gasping).
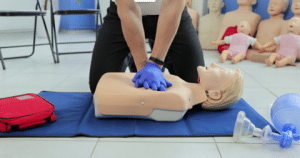
Step-4: Chest Compressions
If the victim is not breathing normally or not at all, start chest compressions.
Kneel down beside the victim, place the heel of one hand on the center of their chest, just below the nipple line.
Place the other hand on top of firsthand by interlocking your fingers.
Keep your arms straight, your shoulders directly over hands, and your body weight centered over the victim’s chest.
Compress the chest at 2 inches deep at a rate of about 100 to120 compressions per minute. Allow chest to fully recoil between compressions.
Continue compressions until professional help arrives or the victim starts breathing normally.
Step-5: Provide Rescue Breaths
After the 30 compressions (in a 30:2 compression-to-ventilation ratio), give two rescue breaths.
Ensure an open airway by tilting the victim’s head back slightly and lifting chin up.
Pinch the victim’s nose shut and place your mouth over theirs, creating a seal.
Give a breath that lasts about one second and makes the chest rise visibly.
Repeat this process for each set of 30 compressions.
Step-6: Continue CPR
Alternate cycles of 30 chest compressions and two rescue breaths.
Continue CPR until the victim starts breathing, emergency personnel take over, or you are physically unable to continue.
Step-7: Use an AED
If an automated defibrillator is available, follow its voice prompts. Attach the AED pads to the victim’s chest as instructed, and let the AED analyze the heart rhythm. If advised, deliver a shock, and continue CPR.
Step-8: Provide Sustained CPR
If no AED is available, continue CPR without interruption until professional help arrives or the victim shows signs of life.
Complications
Rib Fractures: Chest compressions can sometimes lead to rib fractures or damage to the sternum. This is more likely in older individuals with fragile bones.
Lung and Chest Injuries: Forceful chest compressions may cause lung injuries like pneumothorax (collapsed lung) or hemothorax (blood in the chest cavity). It can also lead to chest wall injuries.
Abdominal Injuries: The pressure from chest compressions can sometimes lead to abdominal injuries, such as liver or spleen damage.
Infections: Performing mouth-to-mouth ventilation can expose the rescuer to potential infections, although the risk is low.
Aspiration: During rescue breaths, there is a risk of stomach contents entering the victim’s airway, leading to aspiration pneumonia.
Misplaced Ventilations: In some cases, the rescuer may unintentionally ventilate into the stomach rather than the lungs.
Cardiac Injuries: Chest compressions can cause cardiac injuries, particularly if the person’s underlying condition includes heart disease.
Fractures: In rare cases, CPR may lead to fractures in the upper extremities of the victim due to pressure exerted by the rescuer.
Dislocations: Joint dislocations, particularly in the shoulders, can occur from the force applied during chest compressions.
»
Home » Procedure » Cardiopulmonary Resuscitation (CPR)
Cardiopulmonary Resuscitation (CPR)
Updated :
December 12, 2025
Cardiopulmonary resuscitation (CPR) is an emergency procedure designed to maintain some blood flow to the heart and brain in a person who is in cardiac arrest. It involves the combination of chest compressions and artificial ventilation to provide oxygen to the body’s vital organs when normal breathing and heart function have stopped.
The origins of CPR trace back to the early 18th century when various techniques were attempted, including blowing smoke into the rectum, or using bellows to stimulate breathing. However, the modern concept of CPR was developed in the mid-20th century.
Kouwenhoven Method: Dr. James Elam and Dr. Peter Safar pioneered the “mouth-to-mouth” resuscitation technique in the 1950s.
Cardiac Massage: Dr. Peter Safar and Dr. James Jude further developed CPR, combining chest compressions with artificial ventilation, known as the “cardiac massage” technique.
CPR as We Know It: In 1960, the American Heart Association (AHA) endorsed the “mouth-to-mouth” method, which soon evolved into the combination of chest compressions and rescue breathing that we recognize as CPR today.
AHA Guidelines: The AHA continues to update guidelines for CPR based on scientific research. They emphasize high-quality chest compressions and early defibrillation in cases of sudden cardiac arrest.
CPR is taught and practiced worldwide, saving countless lives each year. Its fundamental goal is to buy time for professional medical assistance to arrive and provide advanced care for those experiencing cardiac arrest.
Cardiac Arrest: CPR is performed in cases of sudden cardiac arrest, where the heart’s electrical activity becomes chaotic or stops altogether. This can be due to various factors, such as a heart attack, arrhythmias, or other cardiac issues.
Respiratory Arrest: If a person experiences a complete cessation of breathing (respiratory arrest), it is essential to initiate CPR to ensure oxygen is delivered to vital organs, including the brain.
Drowning: In cases of near-drowning or drowning victims, CPR should be initiated immediately if the person is unresponsive and not breathing.
Choking: If a person’s airway is obstructed by a foreign object and results in unconsciousness, CPR is required once the airway is cleared.
Drug Overdose: In the event of a severe drug overdose or poisoning that leads to unconsciousness and loss of breathing or a pulse, CPR may be necessary.
Electrocution: Victims of electrical shock can experience cardiac arrest. CPR should be performed if the person is unresponsive and not breathing.
Suffocation: Cases of suffocation or strangulation may cause unconsciousness and respiratory or cardiac arrest. CPR is required in these situations.
Severe Allergic Reaction (Anaphylaxis): In rare cases, severe allergic reactions (anaphylaxis) can lead to cardiac arrest. CPR should be performed if the person becomes unresponsive and loses a pulse.
Trauma: In traumatic injuries that result in cardiac or respiratory arrest, such as severe head injuries, chest injuries, or accidents causing significant blood loss, CPR may be indicated.
Obvious Signs of Death: If a person has been dead for an extended period, such as rigor mortis (stiffening of the body) or obvious signs of decomposition, resuscitative efforts are unlikely to be effective. In such cases, it may not be appropriate to initiate CPR.
Do-Not-Resuscitate (DNR) Orders: If the person has a valid and properly documented DNR order, healthcare providers and bystanders are legally obligated to respect the patient’s wishes. DNR orders specify that the person does not wish to receive CPR or other resuscitative measures in the cardiac events or respiratory arrest.
Decomposed Body: In cases where the body is significantly decomposed, CPR is unlikely to be effective, and it may not be indicated.
Futility: If there is clear evidence that resuscitation is futile and unlikely to result in a successful outcome, such as severe head trauma with a fixed and dilated pupil, continuing CPR may not be appropriate.
Injuries Incompatible with Life: In some traumatic injuries, such as a complete decapitation, where there is no potential for survival, CPR may be contraindicated.
Return of Spontaneous Circulation (ROSC): The primary goal of CPR is to reestablish a heartbeat and circulation. When CPR is administered promptly and effectively, some individuals may achieve ROSC. This means that their heart starts beating again, and they have a return of vital signs.
Survival to Hospital Admission: Some patients who receive CPR may survive long enough to be admitted to a hospital. The chances of survival increase when high-quality CPR is combined with rapid defibrillation and advanced cardiac life support.
Survival to Hospital Discharge: The goal of CPR is for the patient to survive and be discharged from the hospital with a good neurological outcome. However, this outcome is achieved in a smaller percentage of cases and often depends on factors such as the initial cause of cardiac arrest and the duration of CPR.
Neurological Outcomes: For those who survive cardiac arrest, the quality and duration of CPR, as well as the rapidity of advanced care, can influence their neurological outcome. Some survivors may experience minimal or no neurological deficits, while others may have varying degrees of cognitive or physical impairment.
No ROSC or Survival: Unfortunately, not all patients who receive CPR will achieve ROSC or survive. In some cases, the underlying cause of cardiac arrest is too severe, or CPR is not administered in time to be effective. The decision to terminate CPR may be made in cases where resuscitative efforts are deemed futile.
Complications: CPR can be physically demanding and may lead to complications such as rib fractures, lung injuries, and damage to internal organs. While these complications are possible, they are considered acceptable risks given the life-threatening nature of cardiac arrest.
Protective Gear: Before initiating CPR, ensure you are wearing protective equipment such as gloves and a face shield to reduce the infection transmission and ensure your safety.
Automated External Defibrillator (AED): If available, use an AED to analyze the patient’s heart rhythm and deliver electric shocks if needed. These devices are user-friendly and provide voice prompts for guidance.
CPR Barrier Device: This is a one-way valve mask used to provide rescue breaths while preventing direct contact between the rescuer and the patient’s mouth.
Safety: Ensure the safety of the rescuer and bystanders by assessing the scene for potential dangers. If the environment is unsafe, wait for professionals to arrive or ensure the area is secure before beginning CPR.
Position on a Firm Surface: Lay the patient on a firm, flat surface to provide effective chest compressions. For adults and children, this is typically the ground or a hard floor. For infants, a table or countertop may be suitable.
Supine Position: The patient should be in a supine position (lying on their back) for CPR. This position allows for easier access to the chest for chest compressions and the application of an AED.
Clear the Chest: Ensure the patient’s chest is clear of any obstacles, clothing, or items that may interfere with chest compressions.
Adequate Exposure: For effective chest compressions, the patient’s chest should be exposed. Remove any clothing that covers the chest if necessary.
Correct Hand Placement: For adult CPR, position the heel of one hand on the center of the chest, just below the nipple line. Place the other hand on top of the first hand, interlocking the fingers. For children and infants, use one hand or two fingers, respectively.
AED Attachment: If an AED is available, attach the electrode pads to the patient’s chest as per the manufacturer’s instructions. These pads typically have visual aids for proper placement.
Step-1: Assess the Scene
Ensure the safety of yourself, the victim, and any bystanders.
If the scene is safe, approach the victim and check for responsiveness by tapping and shouting, “Are you okay?”
Step-2: Call for Help
If the victim is unresponsive, immediately call emergency services or ask a bystander to do so.
Step-3: Check for Normal Breathing
Place your ear near the victim’s mouth and nose to listen and feel normal breathing (not gasping).
Step-4: Chest Compressions
If the victim is not breathing normally or not at all, start chest compressions.
Kneel down beside the victim, place the heel of one hand on the center of their chest, just below the nipple line.
Place the other hand on top of firsthand by interlocking your fingers.
Keep your arms straight, your shoulders directly over hands, and your body weight centered over the victim’s chest.
Compress the chest at 2 inches deep at a rate of about 100 to120 compressions per minute. Allow chest to fully recoil between compressions.
Continue compressions until professional help arrives or the victim starts breathing normally.
Step-5: Provide Rescue Breaths
After the 30 compressions (in a 30:2 compression-to-ventilation ratio), give two rescue breaths.
Ensure an open airway by tilting the victim’s head back slightly and lifting chin up.
Pinch the victim’s nose shut and place your mouth over theirs, creating a seal.
Give a breath that lasts about one second and makes the chest rise visibly.
Repeat this process for each set of 30 compressions.
Step-6: Continue CPR
Alternate cycles of 30 chest compressions and two rescue breaths.
Continue CPR until the victim starts breathing, emergency personnel take over, or you are physically unable to continue.
Step-7: Use an AED
If an automated defibrillator is available, follow its voice prompts. Attach the AED pads to the victim’s chest as instructed, and let the AED analyze the heart rhythm. If advised, deliver a shock, and continue CPR.
Step-8: Provide Sustained CPR
If no AED is available, continue CPR without interruption until professional help arrives or the victim shows signs of life.
Rib Fractures: Chest compressions can sometimes lead to rib fractures or damage to the sternum. This is more likely in older individuals with fragile bones.
Lung and Chest Injuries: Forceful chest compressions may cause lung injuries like pneumothorax (collapsed lung) or hemothorax (blood in the chest cavity). It can also lead to chest wall injuries.
Abdominal Injuries: The pressure from chest compressions can sometimes lead to abdominal injuries, such as liver or spleen damage.
Infections: Performing mouth-to-mouth ventilation can expose the rescuer to potential infections, although the risk is low.
Aspiration: During rescue breaths, there is a risk of stomach contents entering the victim’s airway, leading to aspiration pneumonia.
Misplaced Ventilations: In some cases, the rescuer may unintentionally ventilate into the stomach rather than the lungs.
Cardiac Injuries: Chest compressions can cause cardiac injuries, particularly if the person’s underlying condition includes heart disease.
Fractures: In rare cases, CPR may lead to fractures in the upper extremities of the victim due to pressure exerted by the rescuer.
Dislocations: Joint dislocations, particularly in the shoulders, can occur from the force applied during chest compressions.
Both our subscription plans include Free CME/CPD AMA PRA Category 1 credits.
Digital Certificate PDF
On course completion, you will receive a full-sized presentation quality digital certificate.
medtigo Simulation
A dynamic medical simulation platform designed to train healthcare professionals and students to effectively run code situations through an immersive hands-on experience in a live, interactive 3D environment.
medtigo Points
medtigo points is our unique point redemption system created to award users for interacting on our site. These points can be redeemed for special discounts on the medtigo marketplace as well as towards the membership cost itself.
Community Forum post/reply = 5 points
*Redemption of points can occur only through the medtigo marketplace, courses, or simulation system. Money will not be credited to your bank account. 10 points = $1.
All Your Certificates in One Place
When you have your licenses, certificates and CMEs in one place, it's easier to track your career growth. You can easily share these with hospitals as well, using your medtigo app.