Ear lacerations are commonly result from trauma, sports injuries, and bites.
The auricle forms from 6 tubercles to create various structures of the external ear.
Intrinsic and extrinsic musculature of the ear is not significantly important.
The ear has vascular skin over cartilaginous framework. Ear lacerations can affect skin, fibrocartilage, or fatty auricle tissues.
Superficial temporal and posterior auricular arteries supply ear blood. If properly repaired ear lacerations heal well due to strong blood supply.
A vascular pedicle with the upper auricular branch supplies sufficient blood to the ear.
Wound management for ear lacerations aims to cover cartilage and reduce hematoma.
Indications
Full-thickness lacerations
Poor wound alignment or cosmetic concern
Contaminated or bite wounds
Bleeding control
Cartilage injury or exposure
Tissue avulsion or flap laceration
Contraindications
Large overlying skin avulsion
Severe crush injuries
Complete or near-complete avulsions
Auricular hematomas
Large cartilage defects
Obvious tissue devitalization
Outcomes
The good cosmetic results when cartilage and skin are aligned properly.
Especially when fine sutures and layered closure techniques are used.
Normal hearing if external auditory canal is not involved. If bolster dressings and antibiotics are used appropriately.
Crush injuries or compromised blood supply can lead to serious ear cartilage infections from bites.
Equipment required
Sterile gloves and drapes
Needle holder
Tissue forceps
Iris scissors or fine surgical scissors
Mosquito hemostats
Absorbable sutures
Non-absorbable sutures
Suture removal kit
Sterile gauze and tape
Non-adherent dressing
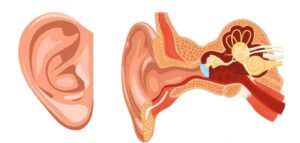
Anatomy of ear
Patient Preparation
Debridement of devitalized tissue is crucial for bite wounds.
Wound infection rates were similar with tap water and sterile saline irrigation.
Gauze can provide comfort before ear canal irrigation. Ensure sterility during wound preparation.
For small ear wounds without cartilage damage and local infiltration is recommended for treatment. Regional nerve blocks are preferred for significant ear laceration anesthesia.
Smaller-gauge needles and slow administration reduce pain from local anesthesia injections.
Epinephrine is traditionally avoided in ear anesthesia due to ischemic necrosis concerns.
Informed Consent:
The provider must encourage patients to ask questions, address concerns, and ensure they understand the repair for informed decision-making.
Patient should be informed about potential procedure failure and necessary additional treatments.
Counsel the patient about possible procedure failure and additional requirements.
Patient Positioning
For lateral decubitus position with injured ear up. Supine position with head rotation may be utilized.
Ear Laceration
Technique
Step 1: Cartilage Approximation
Avascular cartilage needs skin coverage or debridement for survival due to lack of blood supply.
If skin not able to cover cartilage, then cut cartilage from wound margin for skin closure.
A wedge excision technique may be used for non-approximating linear lacerations of the pinna.
A No. 15 scalpel removes a triangular section from the antihelix.
1-mm skin overhang beyond cartilage allows for eversion during closure.
Reattaching avulsed pinna parts after bite wounds is usually inadvisable.
Extensive wounds may require separate cartilage using a 2-layer technique. It is used for large lesions to reduce tension on wound edges.
Start suturing with 5-0 or 6-0 absorbable sutures including only the perichondrium to prevent damage. First sutures should be placed in folds and ridges.
Step 2: Skin closure
Skin usually closed with simple interrupted sutures. Use loose approximation also debride devitalized skin in contaminated wounds.
Close the posterior skin first, then the anterior and lateral surfaces of the helix using 5-0 or 6-0 sutures.
Vertical mattress sutures enhance eversion and appearance for ear rim lacerations. Sutures must go through skin and perichondrium only.
Ear skin and cartilage bond tightly to makes separate closure of cartilage unnecessary.
Step 3: Dressing
After repair, fill ear crevices with Xeroform strips and cover with gauze behind and over the ear.
Apply pressure dressing to prevent hematoma. Wrap head and injured ear with Kling and elastic bandage.
Unaffected ear should remain undressed.
Step 4: Aftercare
Elevate head and avoid exertion or trauma for several days.
Reassess wound in 24 hours for hematoma. Sutures should remove in 4-5 days.
Ear lacerations are commonly result from trauma, sports injuries, and bites.
The auricle forms from 6 tubercles to create various structures of the external ear.
Intrinsic and extrinsic musculature of the ear is not significantly important.
The ear has vascular skin over cartilaginous framework. Ear lacerations can affect skin, fibrocartilage, or fatty auricle tissues.
Superficial temporal and posterior auricular arteries supply ear blood. If properly repaired ear lacerations heal well due to strong blood supply.
A vascular pedicle with the upper auricular branch supplies sufficient blood to the ear.
Wound management for ear lacerations aims to cover cartilage and reduce hematoma.
Full-thickness lacerations
Poor wound alignment or cosmetic concern
Contaminated or bite wounds
Bleeding control
Cartilage injury or exposure
Tissue avulsion or flap laceration
Large overlying skin avulsion
Severe crush injuries
Complete or near-complete avulsions
Auricular hematomas
Large cartilage defects
Obvious tissue devitalization
The good cosmetic results when cartilage and skin are aligned properly.
Especially when fine sutures and layered closure techniques are used.
Normal hearing if external auditory canal is not involved. If bolster dressings and antibiotics are used appropriately.
Crush injuries or compromised blood supply can lead to serious ear cartilage infections from bites.
Sterile gloves and drapes
Needle holder
Tissue forceps
Iris scissors or fine surgical scissors
Mosquito hemostats
Absorbable sutures
Non-absorbable sutures
Suture removal kit
Sterile gauze and tape
Non-adherent dressing
Anatomy of ear
Debridement of devitalized tissue is crucial for bite wounds.
Wound infection rates were similar with tap water and sterile saline irrigation.
Gauze can provide comfort before ear canal irrigation. Ensure sterility during wound preparation.
For small ear wounds without cartilage damage and local infiltration is recommended for treatment. Regional nerve blocks are preferred for significant ear laceration anesthesia.
Smaller-gauge needles and slow administration reduce pain from local anesthesia injections.
Epinephrine is traditionally avoided in ear anesthesia due to ischemic necrosis concerns.
Informed Consent:
The provider must encourage patients to ask questions, address concerns, and ensure they understand the repair for informed decision-making.
Patient should be informed about potential procedure failure and necessary additional treatments.
Counsel the patient about possible procedure failure and additional requirements.
For lateral decubitus position with injured ear up. Supine position with head rotation may be utilized.
Ear Laceration
Step 1: Cartilage Approximation
Avascular cartilage needs skin coverage or debridement for survival due to lack of blood supply.
If skin not able to cover cartilage, then cut cartilage from wound margin for skin closure.
A wedge excision technique may be used for non-approximating linear lacerations of the pinna.
A No. 15 scalpel removes a triangular section from the antihelix.
1-mm skin overhang beyond cartilage allows for eversion during closure.
Reattaching avulsed pinna parts after bite wounds is usually inadvisable.
Extensive wounds may require separate cartilage using a 2-layer technique. It is used for large lesions to reduce tension on wound edges.
Start suturing with 5-0 or 6-0 absorbable sutures including only the perichondrium to prevent damage. First sutures should be placed in folds and ridges.
Step 2: Skin closure
Skin usually closed with simple interrupted sutures. Use loose approximation also debride devitalized skin in contaminated wounds.
Close the posterior skin first, then the anterior and lateral surfaces of the helix using 5-0 or 6-0 sutures.
Vertical mattress sutures enhance eversion and appearance for ear rim lacerations. Sutures must go through skin and perichondrium only.
Ear skin and cartilage bond tightly to makes separate closure of cartilage unnecessary.
Step 3: Dressing
After repair, fill ear crevices with Xeroform strips and cover with gauze behind and over the ear.
Apply pressure dressing to prevent hematoma. Wrap head and injured ear with Kling and elastic bandage.
Unaffected ear should remain undressed.
Step 4: Aftercare
Elevate head and avoid exertion or trauma for several days.
Reassess wound in 24 hours for hematoma. Sutures should remove in 4-5 days.
Both our subscription plans include Free CME/CPD AMA PRA Category 1 credits.
Digital Certificate PDF
On course completion, you will receive a full-sized presentation quality digital certificate.
medtigo Simulation
A dynamic medical simulation platform designed to train healthcare professionals and students to effectively run code situations through an immersive hands-on experience in a live, interactive 3D environment.
medtigo Points
medtigo points is our unique point redemption system created to award users for interacting on our site. These points can be redeemed for special discounts on the medtigo marketplace as well as towards the membership cost itself.
Community Forum post/reply = 5 points
*Redemption of points can occur only through the medtigo marketplace, courses, or simulation system. Money will not be credited to your bank account. 10 points = $1.
All Your Certificates in One Place
When you have your licenses, certificates and CMEs in one place, it's easier to track your career growth. You can easily share these with hospitals as well, using your medtigo app.