Laryngeal Mask Airways (LMA) is a medical device which maintains good airway flow and provides positive pressure ventilation.
Dr. Archie Brain, who recognized this device in 1981 as a safer and better option than endotracheal intubation.
The device is designed in form of elliptical mask attached to a tube that seals around the laryngeal inlet. This allows ventilation without tracheal tube insertion.
LMA is useful in various settings including the operation room, ED, and pre-hospital care due to its handling and speed. Success rate for LMA placement is nearly 100% in the operating room but it has lower rate in emergency settings.
The use of airway ventilation device reduces risk of gastric distention and aspiration, which is more crucial in non-fasted patients.
Indications
It is used in anesthesia for spontaneous and controlled ventilation during surgeries.
These are preferred for short surgeries due to quick insertion and removal of airway device.
LMA are used for failed intubation, which provide effective and rapid ventilation. It is a suitable option for intubation in cardiac arrest cases.
LMA can help to manage airways when positioning does not allow endotracheal intubation in patients.
Contraindications
This device is not for patients with upper airway obstruction as they need to ventilate laryngeal inlet.
LMAs are not suitable for patients who do not maintain oxygen or ventilation with proper placement.
They are not recommended for patients with conditions increasing airway trauma risk during insertion and removal.
Absolute contraindications are inability to open mouth and full airway blockage.
Patients with inadequate sedation, agitation, or altered mental status are not suitable for LMA placement.
It is contraindicated in following conditions:
Prolonged bag-valve-mask ventilation
Morbid obesity
Second or third trimester of pregnancy
Upper gastrointestinal bleed
Outcomes
Successful placement of LMA ensures open airway, provides proper breathing and oxygen intake under anesthesia or emergencies.
LMA have lower aspiration risk than endotracheal tubes when properly used, especially in patients with gastric issues.
LMAs may provide more comfort over endotracheal tubes post-anesthesia.
It reduced discomfort and pain during intubation thus all patients are fully satisfied with this device’s results.
Equipment
Laryngeal Mask Airways
Suction Device
Lubricant
Syringe for Cuff Inflation
End-Tidal CO2 Detector
Patient Preparation
Patient Positioning:
Patient positioned in supine position with head in neutral alignment for LMA insertion.
Proper support to the head and neck should be given for optimal airway alignment and to avoid any risk during the procedure.
Technique
Step 1: Preparation of LMA:
Arrange LMA cuff, balloon, and inflation system at one place. Deflate cuff fully before insertion and prevent any kind of twisting.
Step 2: Insertion of LMA
Use index finger on nondominant hand to guide LMA into mouth then apply lubricant to mask for easier insertion.
Insert LMA along mouth midline, following palate curve. Then proceed steadily until resistance is felt, which indicates correct placement in oropharynx.
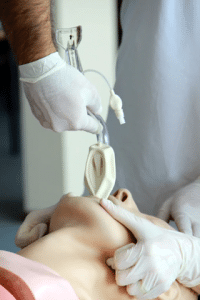
classic type of Laryngeal mask airway
Insertion of Laryngeal mask airway
Step 3: Check Cuff Inflation and seal
Position LMA correctly, then inflate the cuff with appropriate air volume.
Confirm correct placement by checking chest spread and lung sounds.
Step 4: Final confirmation
Surgeons should double check for proper placement of device and monitor level of tidal volume and end-tidal CO2.
Complications
Incorrect handling of the device may lead to airway damage.
E.g., abrasions and lacerations
LMA insertion in the operation room can cause rare complications.
The complication rate was 0.15% in a large study, but it may be higher in emergencies cases.
Airway irritation or sympathetic nervous system stimulation during LMA trigger bronchospasm.
Laryngeal Mask Airways (LMA) is a medical device which maintains good airway flow and provides positive pressure ventilation.
Dr. Archie Brain, who recognized this device in 1981 as a safer and better option than endotracheal intubation.
The device is designed in form of elliptical mask attached to a tube that seals around the laryngeal inlet. This allows ventilation without tracheal tube insertion.
LMA is useful in various settings including the operation room, ED, and pre-hospital care due to its handling and speed. Success rate for LMA placement is nearly 100% in the operating room but it has lower rate in emergency settings.
The use of airway ventilation device reduces risk of gastric distention and aspiration, which is more crucial in non-fasted patients.
It is used in anesthesia for spontaneous and controlled ventilation during surgeries.
These are preferred for short surgeries due to quick insertion and removal of airway device.
LMA are used for failed intubation, which provide effective and rapid ventilation. It is a suitable option for intubation in cardiac arrest cases.
LMA can help to manage airways when positioning does not allow endotracheal intubation in patients.
This device is not for patients with upper airway obstruction as they need to ventilate laryngeal inlet.
LMAs are not suitable for patients who do not maintain oxygen or ventilation with proper placement.
They are not recommended for patients with conditions increasing airway trauma risk during insertion and removal.
Absolute contraindications are inability to open mouth and full airway blockage.
Patients with inadequate sedation, agitation, or altered mental status are not suitable for LMA placement.
It is contraindicated in following conditions:
Prolonged bag-valve-mask ventilation
Morbid obesity
Second or third trimester of pregnancy
Upper gastrointestinal bleed
Successful placement of LMA ensures open airway, provides proper breathing and oxygen intake under anesthesia or emergencies.
LMA have lower aspiration risk than endotracheal tubes when properly used, especially in patients with gastric issues.
LMAs may provide more comfort over endotracheal tubes post-anesthesia.
It reduced discomfort and pain during intubation thus all patients are fully satisfied with this device’s results.
Laryngeal Mask Airways
Suction Device
Lubricant
Syringe for Cuff Inflation
End-Tidal CO2 Detector
Patient Positioning:
Patient positioned in supine position with head in neutral alignment for LMA insertion.
Proper support to the head and neck should be given for optimal airway alignment and to avoid any risk during the procedure.
Step 1: Preparation of LMA:
Arrange LMA cuff, balloon, and inflation system at one place. Deflate cuff fully before insertion and prevent any kind of twisting.
Step 2: Insertion of LMA
Use index finger on nondominant hand to guide LMA into mouth then apply lubricant to mask for easier insertion.
Insert LMA along mouth midline, following palate curve. Then proceed steadily until resistance is felt, which indicates correct placement in oropharynx.
classic type of Laryngeal mask airway
Insertion of Laryngeal mask airway
Step 3: Check Cuff Inflation and seal
Position LMA correctly, then inflate the cuff with appropriate air volume.
Confirm correct placement by checking chest spread and lung sounds.
Step 4: Final confirmation
Surgeons should double check for proper placement of device and monitor level of tidal volume and end-tidal CO2.
Incorrect handling of the device may lead to airway damage.
E.g., abrasions and lacerations
LMA insertion in the operation room can cause rare complications.
The complication rate was 0.15% in a large study, but it may be higher in emergencies cases.
Airway irritation or sympathetic nervous system stimulation during LMA trigger bronchospasm.
Both our subscription plans include Free CME/CPD AMA PRA Category 1 credits.
Digital Certificate PDF
On course completion, you will receive a full-sized presentation quality digital certificate.
medtigo Simulation
A dynamic medical simulation platform designed to train healthcare professionals and students to effectively run code situations through an immersive hands-on experience in a live, interactive 3D environment.
medtigo Points
medtigo points is our unique point redemption system created to award users for interacting on our site. These points can be redeemed for special discounts on the medtigo marketplace as well as towards the membership cost itself.
Community Forum post/reply = 5 points
*Redemption of points can occur only through the medtigo marketplace, courses, or simulation system. Money will not be credited to your bank account. 10 points = $1.
All Your Certificates in One Place
When you have your licenses, certificates and CMEs in one place, it's easier to track your career growth. You can easily share these with hospitals as well, using your medtigo app.