Septal myectomy is a surgery for hypertrophic cardiomyopathy with left ventricular outflow tract obstruction.
It is open-heart surgery to remove thickened septum between the heart’s ventricles.
Hypertrophic cardiomyopathy causes abnormal thickening of heart muscle genetically. Thickening obstructs blood flow from left ventricle to aorta.
Surgical techniques and perioperative care advancements have enhanced septal myectomy’s safety and effectiveness.
It removes thickened septal myocardium to relieve LVOT obstruction and decrease mitral regurgitation.
It improves symptoms while reducing mitral valve regurgitation from systolic anterior motion.
Indications
Septal myectomy is indicated for patients with hypertrophic obstructive cardiomyopathy.
Myectomy outperforms ASA for massive septal hypertrophy with possible midventricular obstruction.
Left Ventricular Outflow Tract Obstruction
Ineffectiveness of Non-Surgical Treatments
Contraindications
Non-Obstructive Hypertrophic Cardiomyopathy
Advanced Heart Failure
Elderly Patients with High Surgical Risk
Coexisting Severe Mitral Valve Disease
Outcomes
LV reverse remodelling occurs in all myocardium layers at the myectomy site and free wall. It includes age, disease extent, myectomy thickness, and LVOT relief.
MRI studies indicated improved apical and midventricular systolic twist post-myectomy, with unchanged basal rotations.
Experienced surgeons achieve <1% mortality in isolated septal myectomy.
Long-term outcome data from several surgical centres spans decades of patient follow-up.
Despite the high demand and proven efficacy of surgical myectomy this may stem from insufficient skills and experience.
Equipment required
Cardiopulmonary Bypass System
Transesophageal Echocardiography Probe
Hemodynamic Monitoring
Electrocardiogram
Median Sternotomy Set
Vascular Clamps
Rongeurs
Surgical Retractors
Valve Sizers and Dilators
Patient Preparation
It includes medical history and diagnostic tests as part of patient preparation.
Informed Consent:
Explain the procedure’s purpose, risks, and potential complications clearly to the patient or guardians.
Patient Positioning
Patient under general anaesthesia in supine position for procedure.
Septal myectomy
Technique
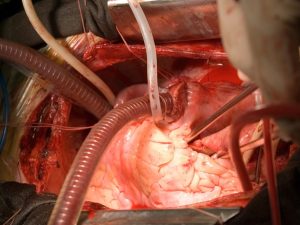
Step 1: Surgical Access
A median sternotomy should be performed to access the heart.
Cardiopulmonary bypass is established with cannulation of the aorta and right atrium.
Step 2: Cardiac Arrest and Exposure
The heart is arrested using cold cardioplegia. Then the aorta is cross-clamped, and the ascending aorta is incised to expose the aortic valve.
Step 3: Visualization of the Septum
A direct line of sight into the left ventricle is achieved through the aortic valve.
Step 4: Resection of Hypertrophied Septum
Then the thickened portion of the septum is removed. A scalpel or surgical rongeur is used to excise muscle while preserving the conduction system.
Step 5: Mitral Valve Assessment
Systolic anterior motion of the mitral valve and mitral regurgitation are reassessed after septal resection.
Step 6: Hemodynamic Evaluation
After completion of the resection, the heart is restarted.
Septal myectomy is a surgery for hypertrophic cardiomyopathy with left ventricular outflow tract obstruction.
It is open-heart surgery to remove thickened septum between the heart’s ventricles.
Hypertrophic cardiomyopathy causes abnormal thickening of heart muscle genetically. Thickening obstructs blood flow from left ventricle to aorta.
Surgical techniques and perioperative care advancements have enhanced septal myectomy’s safety and effectiveness.
It removes thickened septal myocardium to relieve LVOT obstruction and decrease mitral regurgitation.
It improves symptoms while reducing mitral valve regurgitation from systolic anterior motion.
Septal myectomy is indicated for patients with hypertrophic obstructive cardiomyopathy.
Myectomy outperforms ASA for massive septal hypertrophy with possible midventricular obstruction.
Left Ventricular Outflow Tract Obstruction
Ineffectiveness of Non-Surgical Treatments
Non-Obstructive Hypertrophic Cardiomyopathy
Advanced Heart Failure
Elderly Patients with High Surgical Risk
Coexisting Severe Mitral Valve Disease
LV reverse remodelling occurs in all myocardium layers at the myectomy site and free wall. It includes age, disease extent, myectomy thickness, and LVOT relief.
MRI studies indicated improved apical and midventricular systolic twist post-myectomy, with unchanged basal rotations.
Experienced surgeons achieve <1% mortality in isolated septal myectomy.
Long-term outcome data from several surgical centres spans decades of patient follow-up.
Despite the high demand and proven efficacy of surgical myectomy this may stem from insufficient skills and experience.
Cardiopulmonary Bypass System
Transesophageal Echocardiography Probe
Hemodynamic Monitoring
Electrocardiogram
Median Sternotomy Set
Vascular Clamps
Rongeurs
Surgical Retractors
Valve Sizers and Dilators
It includes medical history and diagnostic tests as part of patient preparation.
Informed Consent:
Explain the procedure’s purpose, risks, and potential complications clearly to the patient or guardians.
Patient under general anaesthesia in supine position for procedure.
Septal myectomy
Step 1: Surgical Access
A median sternotomy should be performed to access the heart.
Cardiopulmonary bypass is established with cannulation of the aorta and right atrium.
Step 2: Cardiac Arrest and Exposure
The heart is arrested using cold cardioplegia. Then the aorta is cross-clamped, and the ascending aorta is incised to expose the aortic valve.
Step 3: Visualization of the Septum
A direct line of sight into the left ventricle is achieved through the aortic valve.
Step 4: Resection of Hypertrophied Septum
Then the thickened portion of the septum is removed. A scalpel or surgical rongeur is used to excise muscle while preserving the conduction system.
Step 5: Mitral Valve Assessment
Systolic anterior motion of the mitral valve and mitral regurgitation are reassessed after septal resection.
Step 6: Hemodynamic Evaluation
After completion of the resection, the heart is restarted.
Both our subscription plans include Free CME/CPD AMA PRA Category 1 credits.
Digital Certificate PDF
On course completion, you will receive a full-sized presentation quality digital certificate.
medtigo Simulation
A dynamic medical simulation platform designed to train healthcare professionals and students to effectively run code situations through an immersive hands-on experience in a live, interactive 3D environment.
medtigo Points
medtigo points is our unique point redemption system created to award users for interacting on our site. These points can be redeemed for special discounts on the medtigo marketplace as well as towards the membership cost itself.
Community Forum post/reply = 5 points
*Redemption of points can occur only through the medtigo marketplace, courses, or simulation system. Money will not be credited to your bank account. 10 points = $1.
All Your Certificates in One Place
When you have your licenses, certificates and CMEs in one place, it's easier to track your career growth. You can easily share these with hospitals as well, using your medtigo app.