Arthrocentesis is a medical procedure that involves the aspiration of synovial fluid from a joint capsule for diagnostic or therapeutic purposes. It is also commonly known as Joint Aspiration.
Arthrocentesis is used as a diagnostic tool to help identify the underlying cause of joint symptoms, such as pain, swelling, and inflammation.
It can be used therapeutically to relieve pain and pressure within a joint by removing excess synovial fluid.
Despite the anatomical complexity of the wrist joint, the radiocarpal joint, which may be accessed dorsally, communicates with the majority of the intercarpal spaces.
Joints in the body are enclosed in a capsule and contain a small amount of synovial fluid. This fluid acts as a lubricant, reducing friction between the joint surfaces and providing nourishment to the joint tissues.
Indications
Diagnostic indications are:
Suspicion of crystal arthritis or hemarthrosis
Suspicion of septic arthritis
Imaging studies
Differentiation of inflammatory and non-inflammatory arthritis
Synovial biopsy
Therapeutic indications are:
Injection of corticosteroids and other intra-articular therapies
Lavage of the joint
Removal of tense effusions to relieve pain and improve function
Removal of blood or pus from a joint
Contraindications
Overlying infection at puncture site
Prosthetic joint
Uncontrolled bleeding disorders
Bleeding tendency/anticoagulant therapy
Prosthetic heart valves or immunocompromised patients
Joint ankylosis or severe deformity
Previous total wrist arthroplasty
Outcomes
Arthrocentesis is often used as a diagnostic tool to help identify the underlying cause of joint symptoms.
Arthrocentesis can provide immediate pain relief in cases of large joint effusions (fluid accumulations) by reducing pressure within the joint. This is especially beneficial in conditions like septic arthritis and gout.
Arthrocentesis can help alleviate joint swelling and effusion by removing excess synovial fluid, improving joint function and comfort.
Equipment required
Sterile gloves
Antiseptic solution
Sterile drapes
Sterile gauze
Syringes and needles
A sterile container for collected synovial fluid
Sterile collection tubes for synovial fluid
Antiseptic solution for skin preparation
Patient Preparation
With a little needle, 1% or 2% lidocaine can be injected into the skin and subcutaneous tissues to reach the level of the joint capsule or periarticular lesion for local anesthetic.
Because it is challenging to anesthetize the capsule, this is frequently suitable for joint aspiration. The application of local anaesthetic may be far more unpleasant than a single needle push.
Informed Consent:
Explain the procedure to the patient, including its purpose, potential risks, and benefits.
Obtain informed consent, ensuring the patient fully understands and agrees to the procedure.
Patient Positioning
The patient should be put in a recumbent or comfortable supine posture. This promotes relaxation and prevents fainting.
For the process to be performed more easily, the wrist should be somewhat palmar flexed.
It is necessary to use an antiseptic substance to thoroughly cleanse the skin. It is necessary to mark the needle site and identify bones and other features by palpation before proceeding.
Technique
Place the needle just ulnar to the anatomic snuff box and dorsally, just distal to the radius.
Aim the needle at the skin at a perpendicular angle. Pull the needle back and reroute it slightly in the direction of the thumb if bone gets struck.
When done correctly, the needle enters the joint with a “pop” and moves easily through the extra-articular tissues.
The size of the needle, fluid viscosity, degree of effusion, and presence of fibrin clots all affect how easily the fluid may be removed.
Fluid flow is frequently abruptly stopped when debris or synovial membrane clogs the needle end. To clear the needle and remove more fluid, it is frequently helpful to rotate the needle, withdraw it slightly, or even inject a little amount of fluid again.
A needle that is 1.25 to 2.5 cm long and 22 to 25 gauge is generally sufficient. Sometimes it’s better to use a 20-gauge or even an 18-gauge needle. If necessary, 0.5 mL of steroid may be injected into the area after up to 3-5 mL of fluid has been aspirated from the wrist.
The needle should be quickly removed at the conclusion of any injection process, and the area where the needle was inserted should be lightly compressed.
Bedside ultrasonography (US) can assist locate the best location for needle insertion, which makes it a potential complement to joint aspiration.
US may assist in distinguishing between periarticular illness and joint effusion. The needle implantation location has also been localized using fluoroscopy.
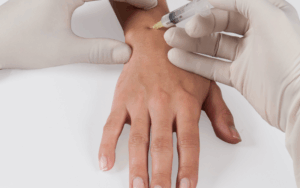
Figure 1. Wrist Arthrocentesis
Complications
Pain at puncture site
Bleeding/Hemarthrosis
Injury to tendons, nerves, or vessels
Vasovagal reaction/syncope during or after procedure
Allergic reaction to local anesthetic or antiseptic agent
Arthrocentesis is a medical procedure that involves the aspiration of synovial fluid from a joint capsule for diagnostic or therapeutic purposes. It is also commonly known as Joint Aspiration.
Arthrocentesis is used as a diagnostic tool to help identify the underlying cause of joint symptoms, such as pain, swelling, and inflammation.
It can be used therapeutically to relieve pain and pressure within a joint by removing excess synovial fluid.
Despite the anatomical complexity of the wrist joint, the radiocarpal joint, which may be accessed dorsally, communicates with the majority of the intercarpal spaces.
Joints in the body are enclosed in a capsule and contain a small amount of synovial fluid. This fluid acts as a lubricant, reducing friction between the joint surfaces and providing nourishment to the joint tissues.
Diagnostic indications are:
Suspicion of crystal arthritis or hemarthrosis
Suspicion of septic arthritis
Imaging studies
Differentiation of inflammatory and non-inflammatory arthritis
Synovial biopsy
Therapeutic indications are:
Injection of corticosteroids and other intra-articular therapies
Lavage of the joint
Removal of tense effusions to relieve pain and improve function
Removal of blood or pus from a joint
Overlying infection at puncture site
Prosthetic joint
Uncontrolled bleeding disorders
Bleeding tendency/anticoagulant therapy
Prosthetic heart valves or immunocompromised patients
Joint ankylosis or severe deformity
Previous total wrist arthroplasty
Arthrocentesis is often used as a diagnostic tool to help identify the underlying cause of joint symptoms.
Arthrocentesis can provide immediate pain relief in cases of large joint effusions (fluid accumulations) by reducing pressure within the joint. This is especially beneficial in conditions like septic arthritis and gout.
Arthrocentesis can help alleviate joint swelling and effusion by removing excess synovial fluid, improving joint function and comfort.
Sterile gloves
Antiseptic solution
Sterile drapes
Sterile gauze
Syringes and needles
A sterile container for collected synovial fluid
Sterile collection tubes for synovial fluid
Antiseptic solution for skin preparation
With a little needle, 1% or 2% lidocaine can be injected into the skin and subcutaneous tissues to reach the level of the joint capsule or periarticular lesion for local anesthetic.
Because it is challenging to anesthetize the capsule, this is frequently suitable for joint aspiration. The application of local anaesthetic may be far more unpleasant than a single needle push.
Informed Consent:
Explain the procedure to the patient, including its purpose, potential risks, and benefits.
Obtain informed consent, ensuring the patient fully understands and agrees to the procedure.
The patient should be put in a recumbent or comfortable supine posture. This promotes relaxation and prevents fainting.
For the process to be performed more easily, the wrist should be somewhat palmar flexed.
It is necessary to use an antiseptic substance to thoroughly cleanse the skin. It is necessary to mark the needle site and identify bones and other features by palpation before proceeding.
Place the needle just ulnar to the anatomic snuff box and dorsally, just distal to the radius.
Aim the needle at the skin at a perpendicular angle. Pull the needle back and reroute it slightly in the direction of the thumb if bone gets struck.
When done correctly, the needle enters the joint with a “pop” and moves easily through the extra-articular tissues.
The size of the needle, fluid viscosity, degree of effusion, and presence of fibrin clots all affect how easily the fluid may be removed.
Fluid flow is frequently abruptly stopped when debris or synovial membrane clogs the needle end. To clear the needle and remove more fluid, it is frequently helpful to rotate the needle, withdraw it slightly, or even inject a little amount of fluid again.
A needle that is 1.25 to 2.5 cm long and 22 to 25 gauge is generally sufficient. Sometimes it’s better to use a 20-gauge or even an 18-gauge needle. If necessary, 0.5 mL of steroid may be injected into the area after up to 3-5 mL of fluid has been aspirated from the wrist.
The needle should be quickly removed at the conclusion of any injection process, and the area where the needle was inserted should be lightly compressed.
Bedside ultrasonography (US) can assist locate the best location for needle insertion, which makes it a potential complement to joint aspiration.
US may assist in distinguishing between periarticular illness and joint effusion. The needle implantation location has also been localized using fluoroscopy.
Figure 1. Wrist Arthrocentesis
Pain at puncture site
Bleeding/Hemarthrosis
Injury to tendons, nerves, or vessels
Vasovagal reaction/syncope during or after procedure
Allergic reaction to local anesthetic or antiseptic agent
Both our subscription plans include Free CME/CPD AMA PRA Category 1 credits.
Digital Certificate PDF
On course completion, you will receive a full-sized presentation quality digital certificate.
medtigo Simulation
A dynamic medical simulation platform designed to train healthcare professionals and students to effectively run code situations through an immersive hands-on experience in a live, interactive 3D environment.
medtigo Points
medtigo points is our unique point redemption system created to award users for interacting on our site. These points can be redeemed for special discounts on the medtigo marketplace as well as towards the membership cost itself.
Community Forum post/reply = 5 points
*Redemption of points can occur only through the medtigo marketplace, courses, or simulation system. Money will not be credited to your bank account. 10 points = $1.
All Your Certificates in One Place
When you have your licenses, certificates and CMEs in one place, it's easier to track your career growth. You can easily share these with hospitals as well, using your medtigo app.