

Free CME credits
Both our subscription plans include Free CME/CPD AMA PRA Category 1 credits.





Tuberculosis (TB) is a contagious bacterial infection that primarily affects the lungs. It is caused by the bacterium Mycobacterium tuberculosis. The bacteria spreads from person to person through the air, typically when an infected person speaks, coughs, or sneezes.
Individuals’ active TB disease can also spread the infection to others through their bodily fluids. Despite the availability of effective treatments, TB remains a significant public health concern, particularly in developing countries.

Chest x-ray showing dense opacity pleural effusion in the lower left lung of primary pulmonary TB
Pulmonary tuberculosis affects the lungs and often causes symptoms such as a chronic cough that lasts up to 3 weeks or more, chest pain, blood in cough (hemoptysis), weight loss, low-grade fever, and night sweats. When the infection spreads to other parts of the body, it is known as secondary tuberculosis.
It tends to be more severe, with a more significant immune response and the potential for forming cavities in the upper part of the lungs. Active TB disease can also cause the infection to disseminate to other organs, such as the spine, the central nervous system, or the bowel.

Tuberculosis is a preventable and curable disease, but it remains a significant public health threat globally, with an estimated 10 million new cases and 1.6 million deaths yearly. It is the leading cause of death among people living with HIV and is also a significant contributor to antimicrobial resistance.
TB is found worldwide, but it disproportionately affects low- and middle-income countries, with about half of all cases occurring in Bangladesh, China, India, Indonesia, Nigeria, Pakistan, the Philippines, and South Africa.
While it is estimated that about 25% of the global population has been infected with TB, most people will not develop the disease, and some will clear the infection on their own. People who are infected but do not show symptoms of TB cannot transmit the disease to others.

The pathophysiology of tuberculosis involves the infection and colonization of the host by Mycobacterium tuberculosis. This typically occurs through inhalation of the bacteria, which are present in the air when an infected person speaks, coughs, or sneezes.
Once the bacteria enter the body, they are phagocytosed (engulfed) by macrophages, which are present in the lungs and other organs. The bacteria multiply within the macrophages, but they also survive and evade the immune response by secreting enzymes that inhibit the production of reactive oxygen species and other toxic compounds and expressing surface proteins that inhibit phagocytosis.
As the infection progresses, the body mounts an immune response to try to control the spread of the bacteria. This involves the activation of T cells, the production of antibodies, and the release of cytokines and other immune mediators. The immune response can lead to the formation of granulomas and an attempt to isolate them from the rest of the body.
If the immune response is unable to control the infection, the bacteria continue to multiply and spread to other parts of the body, leading to the development of active TB disease. In some cases, the bacteria may also become resistant to the antibiotics used to treat the infection, leading to the emergence of drug-resistant strains of TB.

Multiple gram-positive, rod-shaped, Mycobacterium tuberculosis bacilli
Most people who become infected with M. tuberculosis do not develop the disease. This is because the body’s immune system can contain the infection, a state known as latent TB infection. However, in some individuals, the bacteria can become active and cause TB disease.
Risk factors for developing TB include having a compromised immune system due to HIV infection, diabetes, cancer, living in crowded or poorly ventilated areas, and being exposed to tobacco smoke. People with latent TB infection are at increased risk of developing TB disease if their immune systems become weak or compromised.

CT scan of peritoneal tuberculosis, with thickened omentum and peritoneal surface
Extrapulmonary tuberculosis (EPTB) is a form of tuberculosis that affects organs or tissues outside of the lungs. It can affect any part of the body, including the skin, lymph nodes, abdomen, bones, joints, genitourinary tract, meninges, and heart. EPTB is less common than pulmonary TB, accounting for approximately 20% of all TB cases.
It is often more challenging to diagnose than pulmonary TB because the symptoms may not be as obvious. Symptoms can vary depending on the location and severity of the infection but may include fever, night sweats, weight loss, and swelling or pain in the affected area.
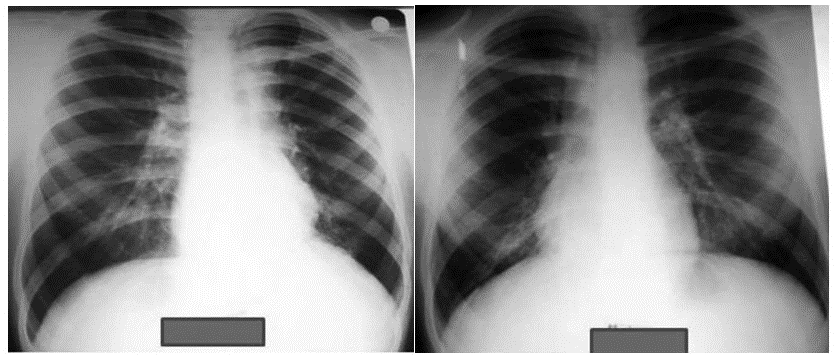
Chest X-rays of a 14-year-old male (BCG-vaccinated) with a positive tuberculin skin test and dextrocardia. Pneumonic infiltration was detected at the follow-up in the right lower zone of the chest X-ray after 50 days of isoniazid treatment
BCG (Bacille Calmette-Guérin) vaccine is a vaccine that is used to protect against tuberculosis. This vaccine is not widely used in the United States. However, it is often given to infants and small children in other countries where TB is common. It primarily affects the lungs but can also infect other parts of the body, such as the lymph nodes, bone, and brain.
The BCG vaccine is not effective in preventing TB, but it can significantly reduce the risk of infection and TB disease, particularly in children. It is essential in areas with a high prevalence of TB, as it can help to reduce the overall incidence in the population. In addition to its role in preventing TB, the BCG vaccine may also have some non-specific effects on the immune system, which may provide some protection against other infections.

The Mantoux skin test
According to the CDC, in the Mantoux test, a standard dose of 5 tuberculin units (TU – 0.1 ml) is injected intradermally on the flexor surface of the left forearm, mid-way between elbow and wrist. The injection should be made with a tuberculin syringe, with the needle bevel facing upward. When placed correctly, the injection should produce a pale wheal of the skin, 6 to 10 mm in diameter. The test result is read after 48–96 hours but 72 hours (3rd day) is ideal.
The response is a classic example of a delayed-type hypersensitivity reaction. T cells and myeloid cells are attracted to the site of reaction in 1–3 days and generate local inflammation. The reaction is read by measuring the diameter of the palpable raised, hardened area across the forearm in millimeters.

The posteroanterior (PA) chest x-ray, revealed pathologic changes in the lung field of a TB patient
TB blood tests are also called interferon-gamma release assays or IGRAs. Two TB blood tests are approved by the U.S. Food and Drug Administration. If the test results are positive, the patient has active or latent TB. If the test results are negative, the patient’s blood did not react to the test, and latent TB is unlikely.
These blood tests are safe during pregnancy. TB blood tests (IGRAs) are not affected by prior BCG vaccination and are not expected to give a false-positive result in individuals who have received BCG. TB blood tests are the preferred method of TB testing for people who have received the BCG vaccine.

M. tuberculosis (stained red) in sputum culture
To detect acid-fast bacilli, it is recommended to conduct sputum smears and cultures on patients producing sputum. Fluorescence microscopy using auramine-rhodamine staining is the preferred method, as it is more sensitive than traditional Ziehl-Neelsen staining.
If a patient is not producing sputum spontaneously, a sample can be induced by inhaling nebulized saline or saline with a bronchodilator solution.

The CT scan at the top reveals the location of two lung cavities, while the bottom PET/CT image shows the failure of a radioactively tagged anti-tb drug (shown as colors) to get inside those cavities and attack the microbes they cover
Drug-Resistant Tuberculosis (DR-TB) is a form of tuberculosis resistant to one or more drugs commonly used, such as isoniazid and rifampicin. It is a serious global health problem because it is more challenging to treat. It can be caused by several factors, including improper treatment of TB, inadequate treatment regimens, and the emergence of M. tuberculosis strains with innate resistance to certain drugs.
RR-TB refers to a type of tuberculosis resistant to rifampicin treatment. This resistance can be detected through genetic or laboratory testing and may or may not be accompanied by resistance to other first-line TB drugs. WHO suggests the use of the 6-month treatment regimen composed of bedaquiline, pretomanid, linezolid, and moxifloxacin (BPaLM) rather than 9-month or longer (18-month) regimens in RR-TB patients.
In patients with confirmed rifampicin-susceptible, treatment with rifampicin, ethambutol, pyrazinamide, and levofloxacin is recommended for 6 months. In patients with confirmed rifampicin-susceptible, it is not recommended to add streptomycin or other injectable agents to the treatment regimen. For patients on longer regimens, the performance of sputum culture and sputum smear microscopy is recommended to monitor treatment response. Sputum culture should be repeated at monthly intervals.

A lung window of a transverse thin-section CT scan (1.25-mm-section thickness) showing multiple cavities in both lungs. [Case of MDR-TB in a 29-year-old man]
Multidrug-Resistant Tuberculosis (MDR-TB) is a type of Drug-Resistant Tuberculosis (DR-TB) that is resistant to at least two of the most effective drugs used to treat TB, such as isoniazid, rifampicin and ethambutol. It is a serious public health concern since it is more challenging to treat and can spread more quickly than drug-sensitive TB.
Several factors, including improper treatment of TB, inadequate treatment regimens, and the emergence of M. tuberculosis strains with innate resistance to certain drugs, can cause MDR-TB. It can affect any part of the body, but it most commonly affects the lungs.
Symptoms of MDR-TB may be similar to those of drug-sensitive TB and may include a persistent cough lasting more than 3 weeks, chest pain, fatigue, weight loss, fever, and swelling of the neck (in case of lymph node involvement). However, the symptoms may be less severe because the bacteria grow more slowly.

HRCT of a patient before and after including levofloxacin, showed improvement of the cavitary lesion in the apical segment of the lower lobe after 15 months
WHO suggests the use of the 6-month treatment regimen composed of bedaquiline, pretomanid, linezolid, and moxifloxacin (BPaLM) rather than 9-month or longer (18-month) regimens in MDR-TB patients. Patients should be included with levofloxacin, moxifloxacin, and linezolid on longer regimens.
Bedaquiline should be included in longer multidrug-resistant TB regimens for patients aged 18 years or more. For patients on longer regimens, a treatment duration of 15–17 months after culture conversion is suggested for most patients; the duration is modified according to the patient’s response to therapy.

An axial thin section of the CT scan shows a large cavity in the left upper lobe. [XDR-TB in 51-year-old non-HIV man]
Extensively Drug-Resistant Tuberculosis (XDR-TB) is a form of drug-resistant tuberculosis that is resistant to at least four of the most effective drugs used to treat TB, such as isoniazid, rifampicin, and any fluoroquinolone, as well as at least one of the injectable second-line TB drugs such as amikacin, kanamycin, or capreomycin. XDR-TB is a serious public health issue because it is extremely difficult to treat and spreads rapidly.
It can be caused by several factors, including improper treatment, inadequate treatment regimens, and the emergence of M. tuberculosis strains with innate resistance to certain drugs. It can affect any part of the body but most commonly affects the lungs. Symptoms of XDR-TB may be similar to those of drug-sensitive TB and may include a persistent cough, chest pain, fatigue, weight loss, and fever. However, the symptoms may be less severe because the bacteria grow slowly.

Congenital Extensively Drug-Resistant Tuberculosis in a 21-day old neonate
XDR-TB is treated with a combination of second-line TB drugs, which are less effective and more toxic than the first-line drugs used to treat drug-sensitive TB.
Treatment regimens for XDR-TB can be complex and may require multiple drugs taken over a period of several months or even years. In some cases, surgery may be necessary to remove infected tissue or to repair damage caused by the infection.

Diffuse nodular infiltration in HIV-TB coinfection in patient with CD4 count less than 200
Individuals with HIV are more prone to be infected with TB, a major cause of death for people with HIV. As HIV impairs the immune system, it is opportunistic for latent TB infection to turn into active TB disease. Without proper treatment, both HIV and TB can significantly shorten lifespan.
Unlike other HIV-associated opportunistic infections, tuberculosis may occur at relatively high levels of CD4 counts. However, its frequency markedly increases in patients with more severe immunosuppression. HIV-TB cases have been observed to have severe immunosuppression at presentation, with several studies reporting CD4 counts of less than 200.
In patients with mild immunosuppression, chest X-ray typically shows upper lobe or bilateral infiltrates, cavitation, pulmonary fibrosis, and shrinkage. The clinical picture often resembles post-primary pulmonary tuberculosis, and the sputum smear is usually positive.

Miliary tuberculosis in a complicated case of drug-resistant tuberculosis
Tuberculosis can cause serious complications, particularly in individuals with a weak immune system or underlying health conditions. Some of the potential complications include extensive damage to the lungs, infection of the membranes surrounding the brain and spinal cord (TB meningitis), and the accumulation of pus in the pleural space around the lungs (empyema).
Other complications include damage to the cervical sympathetic ganglia, which can cause Horner’s syndrome, and the spread of the infection throughout the body (miliary spread or disseminated tuberculosis), which can lead to serious infections in other organs. In severe cases, TB can also cause acute respiratory distress syndrome and pneumothorax, or a collapsed lung. In some cases, it can lead to the development of systemic amyloidosis.

Type 1 respiratory failure in drug-resistant TB
Tuberculosis is a bacterial infection that can be treated effectively with medications, but without treatment, the mortality rate is over 50%.
However, certain groups of people may be at higher risk for worse outcomes or death from TB, including those at the extremes of age, delayed in receiving treatment, those with radiologic evidence of extensive spread of the infection, severe respiratory compromise requiring mechanical ventilation, immunosuppression, and those with multidrug-resistant TB.
It is important for individuals at higher risk for TB or exposed to TB to seek medical attention as soon as possible to receive timely and appropriate treatment.

December 2, 2022

November 7, 2022
Both our subscription plans include Free CME/CPD AMA PRA Category 1 credits.

On course completion, you will receive a full-sized presentation quality digital certificate.

When you have your licenses, certificates and CMEs in one place, it's easier to track your career growth. You can easily share these with hospitals as well, using your medtigo app.



