The epidemiology of Peptococcus asaccharolyticus is not well studied, but some general aspects can be summarized as follows:
Peptococcus asaccharolyticus is a Gram-positive anaerobic cocci (GPAC) type that can cause various human infections, especially in the female genital tract, bones and joints, soft tissues, and blood.
Peptococcus asaccharolyticus is part of the normal flora of the human oral cavity, alimentary tract, skin and vagina. It may cause opportunistic infections when the host defenses are compromised or when the bacteria are introduced into sterile sites.
Peptococcus asaccharolyticus is usually transmitted by endogenous sources, such as dental procedures, intrauterine devices, abortion, or childbirth. Exogenous sources, such as trauma, surgery, or foreign body insertion, may also transmit it.
Peptococcus asaccharolyticus is often found in mixed infections with other anaerobic or aerobic bacteria. It may act synergistically with other pathogens to enhance the virulence and severity of the infection.
Peptococcus asaccharolyticus is usually susceptible to penicillin, metronidazole, clindamycin, and cefoxitin. However, some strains may have reduced susceptibility or resistance to these antibiotics. Therefore, it is essential to perform culture and susceptibility testing for optimal treatment.
Kingdom: Bacteria
Phylum: Bacillota
Class: Clostridia
Order: Eubacteriales
Family: Peptoniphilaceae
Genus: Peptoniphilus
Species: P. asaccharolyticus
The structure of Peptococcus asaccharolyticus, a species of anaerobic, Gram-positive bacteria that can cause infections in humans, especially in the female genital tract, can be summarized in five points as follows:
The cells are small, spherical, and can occur in short chains, pairs, or individually.
The cell wall comprises peptidoglycan and teichoic acids and lacks lipopolysaccharide (LPS) or outer membrane.
The cell membrane contains phospholipids, glycolipids, and cholesterol and has a high fluidity and permeability.
The cytoplasm contains a single circular chromosome, ribosomes, plasmids, and various enzymes and metabolites.
The cells lack flagella, pili, capsules, or spores but may produce extracellular polysaccharides or biofilms.
Peptococcus asaccharolyticus has two antigenic types, A and B, based on the agglutination reaction with specific antisera. The antigenic types are related to the biochemical properties of the bacteria, such as indole production, glucose fermentation, and esculin hydrolysis. Type A strains are indole-positive, glucose-fermenting, and esculin-negative, while type B strains are indole-negative, glucose-nonfermenting, and esculin-positive.
The authors also developed a rapid identification method for Peptococcus asaccharolyticus using a latex agglutination test to distinguish between the two antigenic types.
The pathogenesis of Peptococcus asaccharolyticus, which is now reclassified as Peptoniphilus asaccharolyticus, can be summarized in five points:
Peptococcus asaccharolyticus is part of the normal flora of the human oral cavity, alimentary tract, skin, and vagina. It may cause opportunistic infections when the host defenses are compromised, or the bacteria are introduced into sterile sites.
Peptococcus asaccharolyticus is usually transmitted by endogenous sources, such as dental procedures, intrauterine devices, abortion, or childbirth. Exogenous sources, such as trauma, surgery, or foreign body insertion, may also transmit it.
Peptococcus asaccharolyticus is often found in mixed infections with other anaerobic or aerobic bacteria. It may act synergistically with other pathogens to enhance the virulence and severity of the infection.
Peptococcus asaccharolyticus is usually susceptible to penicillin, metronidazole, clindamycin, and cefoxitin. However, some strains may have reduced susceptibility or resistance to these antibiotics. Therefore, it is essential to perform culture and susceptibility testing for optimal treatment.
The host defenses against Peptococcus asaccharolyticus are not well studied, but they may include the following mechanisms:
The normal flora of the vagina and other mucosal surfaces can compete with Peptococcus asaccharolyticus and prevent its overgrowth or invasion. Some probiotics, such as lactobacilli, may also benefit the vaginal microbiota and inhibit Peptococcus asaccharolyticus.
The epithelial barrier of the mucosa can prevent the attachment and penetration of Peptococcus asaccharolyticus into the underlying tissues. The epithelial cells may also secrete antimicrobial peptides, such as defensins and cathelicidins, that can kill or inhibit Peptococcus asaccharolyticus.
Through various receptors, including toll-like receptors and nucleotide-binding oligomerization domain (NOD )-receptors, the innate immune system can identify and destroy Peptococcus asaccharolyticus.
. These receptors can activate inflammatory responses, such as the production of cytokines, chemokines, and nitric oxide, that can recruit and activate phagocytes, such as neutrophils and macrophages. These phagocytes can engulf and destroy Peptococcus asaccharolyticus by using reactive oxygen species (ROS), lysosomal enzymes, and autophagy.
By creating antibodies and T cells, the adaptive immune system can establish targeted defenses against Peptococcus asaccharolyticus. Antibodies can bind to Peptococcus asaccharolyticus and neutralize its virulence factors, such as hemolysins and proteases. Antibodies can also opsonize Peptococcus asaccharolyticus and enhance its phagocytosis by phagocytes. T cells can help activate B cells and macrophages and directly kill infected cells by releasing cytotoxic molecules.
The clinical manifestations of Peptococcus asaccharolyticus infection are:
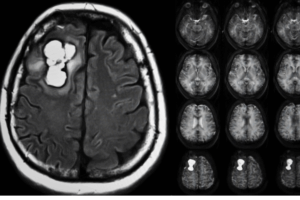
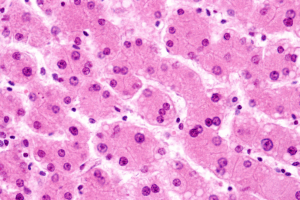
Bacteremia with liver involvement may present with fever, chills, and right upper quadrant abdominal pain. This condition may be associated with dental procedures or other sources of oral infection.
Deep-seated anaerobic soft-tissue infections, such as abscesses, cellulitis, necrotizing fasciitis, and myonecrosis. These infections may occur after trauma, surgery, or foreign body insertion.
Bacterial arthritis and osteomyelitis are two examples of joint and bone infections. These infections may result from hematogenous spread or direct injection of the bacteria into the bone or joint.
female vaginal tract infections like endometritis, pelvic inflammatory disease, tubo-ovarian abscess, and postpartum infection. These infections may be related to intrauterine devices, abortion, or childbirth.
Peptococcus asaccharolyticus is usually susceptible to penicillin, metronidazole, clindamycin, and cefoxitin. However, some strains may have reduced susceptibility or resistance to these antibiotics. Therefore, it is essential to perform culture and susceptibility testing for optimal treatment.
Perform Gram stain: Look for tiny, spherical, non-spore-forming bacteria.
Culture anaerobically on blood agar or thioglycolate broth.
Conduct biochemical tests for type identification (A or B).
Type A: Indole-positive, glucose-fermenting, esculin-negative.
Type B: Indole-negative, glucose-nonfermenting, esculin-positive.
Perform latex agglutination test for rapid typing.
Conduct antimicrobial susceptibility testing:
Susceptible to penicillin, cefoxitin, and clindamycin.
The control of Peptococcus asaccharolyticus, a species of anaerobic, Gram-positive bacteria that can cause infections in humans, especially in the female genital tract, may involve the following measures:
Prevention of exposure to the bacteria by maintaining good hygiene and avoiding sexual contact with infected partners.
Treatment of infections caused by Peptococcus asaccharolyticus with appropriate antibiotics, such as beta-lactams (penicillin, cefoxitin, clindamycin) or metronidazole.
The antibiotic susceptibility of the bacteria should be tested before initiating therapy, as some strains may resist certain drugs.
Management of complications and sequelae of infections, such as abscesses, pelvic inflammatory disease, infertility, and septicemia, by surgical drainage, anti-inflammatory agents, and supportive care.
Enhancement of host immunity and resistance to infections by using probiotics, such as lactobacilli, that can modulate the vaginal microbiota and inhibit the growth of Peptococcus asaccharolyticus.
Peptoniphilus asaccharolyticus – Commensal, pathogen or synergist? Two case reports on invasive Peptoniphilus asaccharolyticus infection – ScienceDirect
Peptoniphilus asaccharolyticus – an overview | ScienceDirect Topics
The epidemiology of Peptococcus asaccharolyticus is not well studied, but some general aspects can be summarized as follows:
Peptococcus asaccharolyticus is a Gram-positive anaerobic cocci (GPAC) type that can cause various human infections, especially in the female genital tract, bones and joints, soft tissues, and blood.
Peptococcus asaccharolyticus is part of the normal flora of the human oral cavity, alimentary tract, skin and vagina. It may cause opportunistic infections when the host defenses are compromised or when the bacteria are introduced into sterile sites.
Peptococcus asaccharolyticus is usually transmitted by endogenous sources, such as dental procedures, intrauterine devices, abortion, or childbirth. Exogenous sources, such as trauma, surgery, or foreign body insertion, may also transmit it.
Peptococcus asaccharolyticus is often found in mixed infections with other anaerobic or aerobic bacteria. It may act synergistically with other pathogens to enhance the virulence and severity of the infection.
Peptococcus asaccharolyticus is usually susceptible to penicillin, metronidazole, clindamycin, and cefoxitin. However, some strains may have reduced susceptibility or resistance to these antibiotics. Therefore, it is essential to perform culture and susceptibility testing for optimal treatment.
Kingdom: Bacteria
Phylum: Bacillota
Class: Clostridia
Order: Eubacteriales
Family: Peptoniphilaceae
Genus: Peptoniphilus
Species: P. asaccharolyticus
The structure of Peptococcus asaccharolyticus, a species of anaerobic, Gram-positive bacteria that can cause infections in humans, especially in the female genital tract, can be summarized in five points as follows:
The cells are small, spherical, and can occur in short chains, pairs, or individually.
The cell wall comprises peptidoglycan and teichoic acids and lacks lipopolysaccharide (LPS) or outer membrane.
The cell membrane contains phospholipids, glycolipids, and cholesterol and has a high fluidity and permeability.
The cytoplasm contains a single circular chromosome, ribosomes, plasmids, and various enzymes and metabolites.
The cells lack flagella, pili, capsules, or spores but may produce extracellular polysaccharides or biofilms.
Peptococcus asaccharolyticus has two antigenic types, A and B, based on the agglutination reaction with specific antisera. The antigenic types are related to the biochemical properties of the bacteria, such as indole production, glucose fermentation, and esculin hydrolysis. Type A strains are indole-positive, glucose-fermenting, and esculin-negative, while type B strains are indole-negative, glucose-nonfermenting, and esculin-positive.
The authors also developed a rapid identification method for Peptococcus asaccharolyticus using a latex agglutination test to distinguish between the two antigenic types.
The pathogenesis of Peptococcus asaccharolyticus, which is now reclassified as Peptoniphilus asaccharolyticus, can be summarized in five points:
Peptococcus asaccharolyticus is part of the normal flora of the human oral cavity, alimentary tract, skin, and vagina. It may cause opportunistic infections when the host defenses are compromised, or the bacteria are introduced into sterile sites.
Peptococcus asaccharolyticus is usually transmitted by endogenous sources, such as dental procedures, intrauterine devices, abortion, or childbirth. Exogenous sources, such as trauma, surgery, or foreign body insertion, may also transmit it.
Peptococcus asaccharolyticus is often found in mixed infections with other anaerobic or aerobic bacteria. It may act synergistically with other pathogens to enhance the virulence and severity of the infection.
Peptococcus asaccharolyticus is usually susceptible to penicillin, metronidazole, clindamycin, and cefoxitin. However, some strains may have reduced susceptibility or resistance to these antibiotics. Therefore, it is essential to perform culture and susceptibility testing for optimal treatment.
The host defenses against Peptococcus asaccharolyticus are not well studied, but they may include the following mechanisms:
The normal flora of the vagina and other mucosal surfaces can compete with Peptococcus asaccharolyticus and prevent its overgrowth or invasion. Some probiotics, such as lactobacilli, may also benefit the vaginal microbiota and inhibit Peptococcus asaccharolyticus.
The epithelial barrier of the mucosa can prevent the attachment and penetration of Peptococcus asaccharolyticus into the underlying tissues. The epithelial cells may also secrete antimicrobial peptides, such as defensins and cathelicidins, that can kill or inhibit Peptococcus asaccharolyticus.
Through various receptors, including toll-like receptors and nucleotide-binding oligomerization domain (NOD )-receptors, the innate immune system can identify and destroy Peptococcus asaccharolyticus.
. These receptors can activate inflammatory responses, such as the production of cytokines, chemokines, and nitric oxide, that can recruit and activate phagocytes, such as neutrophils and macrophages. These phagocytes can engulf and destroy Peptococcus asaccharolyticus by using reactive oxygen species (ROS), lysosomal enzymes, and autophagy.
By creating antibodies and T cells, the adaptive immune system can establish targeted defenses against Peptococcus asaccharolyticus. Antibodies can bind to Peptococcus asaccharolyticus and neutralize its virulence factors, such as hemolysins and proteases. Antibodies can also opsonize Peptococcus asaccharolyticus and enhance its phagocytosis by phagocytes. T cells can help activate B cells and macrophages and directly kill infected cells by releasing cytotoxic molecules.
The clinical manifestations of Peptococcus asaccharolyticus infection are:
Bacteremia with liver involvement may present with fever, chills, and right upper quadrant abdominal pain. This condition may be associated with dental procedures or other sources of oral infection.
Deep-seated anaerobic soft-tissue infections, such as abscesses, cellulitis, necrotizing fasciitis, and myonecrosis. These infections may occur after trauma, surgery, or foreign body insertion.
Bacterial arthritis and osteomyelitis are two examples of joint and bone infections. These infections may result from hematogenous spread or direct injection of the bacteria into the bone or joint.
female vaginal tract infections like endometritis, pelvic inflammatory disease, tubo-ovarian abscess, and postpartum infection. These infections may be related to intrauterine devices, abortion, or childbirth.
Peptococcus asaccharolyticus is usually susceptible to penicillin, metronidazole, clindamycin, and cefoxitin. However, some strains may have reduced susceptibility or resistance to these antibiotics. Therefore, it is essential to perform culture and susceptibility testing for optimal treatment.
Perform Gram stain: Look for tiny, spherical, non-spore-forming bacteria.
Culture anaerobically on blood agar or thioglycolate broth.
Conduct biochemical tests for type identification (A or B).
Type A: Indole-positive, glucose-fermenting, esculin-negative.
Type B: Indole-negative, glucose-nonfermenting, esculin-positive.
Perform latex agglutination test for rapid typing.
Conduct antimicrobial susceptibility testing:
Susceptible to penicillin, cefoxitin, and clindamycin.
The control of Peptococcus asaccharolyticus, a species of anaerobic, Gram-positive bacteria that can cause infections in humans, especially in the female genital tract, may involve the following measures:
Prevention of exposure to the bacteria by maintaining good hygiene and avoiding sexual contact with infected partners.
Treatment of infections caused by Peptococcus asaccharolyticus with appropriate antibiotics, such as beta-lactams (penicillin, cefoxitin, clindamycin) or metronidazole.
The antibiotic susceptibility of the bacteria should be tested before initiating therapy, as some strains may resist certain drugs.
Management of complications and sequelae of infections, such as abscesses, pelvic inflammatory disease, infertility, and septicemia, by surgical drainage, anti-inflammatory agents, and supportive care.
Enhancement of host immunity and resistance to infections by using probiotics, such as lactobacilli, that can modulate the vaginal microbiota and inhibit the growth of Peptococcus asaccharolyticus.
Peptoniphilus asaccharolyticus – Commensal, pathogen or synergist? Two case reports on invasive Peptoniphilus asaccharolyticus infection – ScienceDirect
Peptoniphilus asaccharolyticus – an overview | ScienceDirect Topics
The epidemiology of Peptococcus asaccharolyticus is not well studied, but some general aspects can be summarized as follows:
Peptococcus asaccharolyticus is a Gram-positive anaerobic cocci (GPAC) type that can cause various human infections, especially in the female genital tract, bones and joints, soft tissues, and blood.
Peptococcus asaccharolyticus is part of the normal flora of the human oral cavity, alimentary tract, skin and vagina. It may cause opportunistic infections when the host defenses are compromised or when the bacteria are introduced into sterile sites.
Peptococcus asaccharolyticus is usually transmitted by endogenous sources, such as dental procedures, intrauterine devices, abortion, or childbirth. Exogenous sources, such as trauma, surgery, or foreign body insertion, may also transmit it.
Peptococcus asaccharolyticus is often found in mixed infections with other anaerobic or aerobic bacteria. It may act synergistically with other pathogens to enhance the virulence and severity of the infection.
Peptococcus asaccharolyticus is usually susceptible to penicillin, metronidazole, clindamycin, and cefoxitin. However, some strains may have reduced susceptibility or resistance to these antibiotics. Therefore, it is essential to perform culture and susceptibility testing for optimal treatment.
Kingdom: Bacteria
Phylum: Bacillota
Class: Clostridia
Order: Eubacteriales
Family: Peptoniphilaceae
Genus: Peptoniphilus
Species: P. asaccharolyticus
The structure of Peptococcus asaccharolyticus, a species of anaerobic, Gram-positive bacteria that can cause infections in humans, especially in the female genital tract, can be summarized in five points as follows:
The cells are small, spherical, and can occur in short chains, pairs, or individually.
The cell wall comprises peptidoglycan and teichoic acids and lacks lipopolysaccharide (LPS) or outer membrane.
The cell membrane contains phospholipids, glycolipids, and cholesterol and has a high fluidity and permeability.
The cytoplasm contains a single circular chromosome, ribosomes, plasmids, and various enzymes and metabolites.
The cells lack flagella, pili, capsules, or spores but may produce extracellular polysaccharides or biofilms.
Peptococcus asaccharolyticus has two antigenic types, A and B, based on the agglutination reaction with specific antisera. The antigenic types are related to the biochemical properties of the bacteria, such as indole production, glucose fermentation, and esculin hydrolysis. Type A strains are indole-positive, glucose-fermenting, and esculin-negative, while type B strains are indole-negative, glucose-nonfermenting, and esculin-positive.
The authors also developed a rapid identification method for Peptococcus asaccharolyticus using a latex agglutination test to distinguish between the two antigenic types.
The pathogenesis of Peptococcus asaccharolyticus, which is now reclassified as Peptoniphilus asaccharolyticus, can be summarized in five points:
Peptococcus asaccharolyticus is part of the normal flora of the human oral cavity, alimentary tract, skin, and vagina. It may cause opportunistic infections when the host defenses are compromised, or the bacteria are introduced into sterile sites.
Peptococcus asaccharolyticus is usually transmitted by endogenous sources, such as dental procedures, intrauterine devices, abortion, or childbirth. Exogenous sources, such as trauma, surgery, or foreign body insertion, may also transmit it.
Peptococcus asaccharolyticus is often found in mixed infections with other anaerobic or aerobic bacteria. It may act synergistically with other pathogens to enhance the virulence and severity of the infection.
Peptococcus asaccharolyticus is usually susceptible to penicillin, metronidazole, clindamycin, and cefoxitin. However, some strains may have reduced susceptibility or resistance to these antibiotics. Therefore, it is essential to perform culture and susceptibility testing for optimal treatment.
The host defenses against Peptococcus asaccharolyticus are not well studied, but they may include the following mechanisms:
The normal flora of the vagina and other mucosal surfaces can compete with Peptococcus asaccharolyticus and prevent its overgrowth or invasion. Some probiotics, such as lactobacilli, may also benefit the vaginal microbiota and inhibit Peptococcus asaccharolyticus.
The epithelial barrier of the mucosa can prevent the attachment and penetration of Peptococcus asaccharolyticus into the underlying tissues. The epithelial cells may also secrete antimicrobial peptides, such as defensins and cathelicidins, that can kill or inhibit Peptococcus asaccharolyticus.
Through various receptors, including toll-like receptors and nucleotide-binding oligomerization domain (NOD )-receptors, the innate immune system can identify and destroy Peptococcus asaccharolyticus.
. These receptors can activate inflammatory responses, such as the production of cytokines, chemokines, and nitric oxide, that can recruit and activate phagocytes, such as neutrophils and macrophages. These phagocytes can engulf and destroy Peptococcus asaccharolyticus by using reactive oxygen species (ROS), lysosomal enzymes, and autophagy.
By creating antibodies and T cells, the adaptive immune system can establish targeted defenses against Peptococcus asaccharolyticus. Antibodies can bind to Peptococcus asaccharolyticus and neutralize its virulence factors, such as hemolysins and proteases. Antibodies can also opsonize Peptococcus asaccharolyticus and enhance its phagocytosis by phagocytes. T cells can help activate B cells and macrophages and directly kill infected cells by releasing cytotoxic molecules.
The clinical manifestations of Peptococcus asaccharolyticus infection are:
Bacteremia with liver involvement may present with fever, chills, and right upper quadrant abdominal pain. This condition may be associated with dental procedures or other sources of oral infection.
Deep-seated anaerobic soft-tissue infections, such as abscesses, cellulitis, necrotizing fasciitis, and myonecrosis. These infections may occur after trauma, surgery, or foreign body insertion.
Bacterial arthritis and osteomyelitis are two examples of joint and bone infections. These infections may result from hematogenous spread or direct injection of the bacteria into the bone or joint.
female vaginal tract infections like endometritis, pelvic inflammatory disease, tubo-ovarian abscess, and postpartum infection. These infections may be related to intrauterine devices, abortion, or childbirth.
Peptococcus asaccharolyticus is usually susceptible to penicillin, metronidazole, clindamycin, and cefoxitin. However, some strains may have reduced susceptibility or resistance to these antibiotics. Therefore, it is essential to perform culture and susceptibility testing for optimal treatment.
Perform Gram stain: Look for tiny, spherical, non-spore-forming bacteria.
Culture anaerobically on blood agar or thioglycolate broth.
Conduct biochemical tests for type identification (A or B).
Type A: Indole-positive, glucose-fermenting, esculin-negative.
Type B: Indole-negative, glucose-nonfermenting, esculin-positive.
Perform latex agglutination test for rapid typing.
Conduct antimicrobial susceptibility testing:
Susceptible to penicillin, cefoxitin, and clindamycin.
The control of Peptococcus asaccharolyticus, a species of anaerobic, Gram-positive bacteria that can cause infections in humans, especially in the female genital tract, may involve the following measures:
Prevention of exposure to the bacteria by maintaining good hygiene and avoiding sexual contact with infected partners.
Treatment of infections caused by Peptococcus asaccharolyticus with appropriate antibiotics, such as beta-lactams (penicillin, cefoxitin, clindamycin) or metronidazole.
The antibiotic susceptibility of the bacteria should be tested before initiating therapy, as some strains may resist certain drugs.
Management of complications and sequelae of infections, such as abscesses, pelvic inflammatory disease, infertility, and septicemia, by surgical drainage, anti-inflammatory agents, and supportive care.
Enhancement of host immunity and resistance to infections by using probiotics, such as lactobacilli, that can modulate the vaginal microbiota and inhibit the growth of Peptococcus asaccharolyticus.
Peptoniphilus asaccharolyticus – Commensal, pathogen or synergist? Two case reports on invasive Peptoniphilus asaccharolyticus infection – ScienceDirect
Peptoniphilus asaccharolyticus – an overview | ScienceDirect Topics
Loading...
Free CME credits
Both our subscription plans include Free CME/CPD AMA PRA Category 1 credits.
Digital Certificate PDF
On course completion, you will receive a full-sized presentation quality digital certificate.
medtigo Simulation
A dynamic medical simulation platform designed to train healthcare professionals and students to effectively run code situations through an immersive hands-on experience in a live, interactive 3D environment.
medtigo Points
medtigo points is our unique point redemption system created to award users for interacting on our site. These points can be redeemed for special discounts on the medtigo marketplace as well as towards the membership cost itself.
Community Forum post/reply = 5 points
*Redemption of points can occur only through the medtigo marketplace, courses, or simulation system. Money will not be credited to your bank account. 10 points = $1.
All Your Certificates in One Place
When you have your licenses, certificates and CMEs in one place, it's easier to track your career growth. You can easily share these with hospitals as well, using your medtigo app.